
- Available in Welsh
- About us
- Foreword
- At a glance: How to develop effective HSC-industry partnerships
- About this guidance
- What are NHS-industry partnerships?
- The benefits of working together
- Stage 1 Project identification and scoping
- Stage 2 Project setup and governance structures
- The executive summary
- Stage 3 Project implementation and outcomes reporting
- Key resource: Recommended Summary of Project Outcomes Framework
- Further reading
- Appendices 1 and 2
- Available in Welsh
- About us
- Foreword
- At a glance: How to develop effective HSC-industry partnerships
- About this guidance
- What are NHS-industry partnerships?
- The benefits of working together
- Stage 1 Project identification and scoping
- Stage 2 Project setup and governance structures
- The executive summary
- Stage 3 Project implementation and outcomes reporting
- Key resource: Recommended Summary of Project Outcomes Framework
- Further reading
- Appendices 1 and 2
Available in Welsh
About us
The Welsh NHS Confederation is the only national membership body representing the leaders of the organisations making up the NHS in Wales: the seven local health boards, three NHS trusts and two special health authorities.
We host NHS Wales Employers and are part of the NHS Confederation.
We support our members by acting as a driving force for positive change through strong representation, facilitating system leadership and our proactive policy, influencing, communications, events and engagement work.
To find out more, visit www.nhsconfed.org/wales
The Association of the British Pharmaceutical Industry (ABPI) exists to make the UK the best place in the world to research, develop and access medicines and vaccines to improve patient care.
We represent companies of all sizes that invest in making and discovering medicines and vaccines to enhance and save the lives of millions of people around the world. In England, Scotland, Wales and Northern Ireland, we work in partnership with governments and the NHS so that patients can get new treatments faster and the NHS can plan how much it spends on medicines.
Every day, our members partner with healthcare professionals, academics and patient organisations to find new solutions to unmet health needs.
To find out more, visit www.abpi.org.uk
Foreword
Across Wales, the potential of NHS and industry partnerships to transform health services and improve outcomes for patients has never been greater. A growing body of research confirms that where partnerships take place, they are associated with better health outcomes for patients, improve access to innovation, and create system-wide benefits. The evidence from Wales and beyond is clear: collaboration between the NHS and industry is not just transformational, it is essential.
We have seen this first-hand through the wealth of examples captured in the Association of the British Pharmaceutical Industry’s (ABPI’s) NHS–Industry Partnership Case Studies Library, which features projects from across all four nations of the UK, including many from Wales. These projects demonstrate the ‘triple win’ in action, delivering better outcomes for patients, strengthening NHS capacity and capability, and making responsible use of industry expertise and resources.
This new Welsh guidance is the product of a truly collaborative effort between the Welsh NHS Confederation and the ABPI. It draws together the experiences, insights and lessons from NHS leaders and industry partners into a single, practical resource designed to make partnership working easier, more transparent and more impactful.
Central to the guidance are new, jointly endorsed frameworks and sources of assurance that support every stage of the partnership lifecycle, from identifying opportunities and scoping a project, through governance and delivery, to reporting outcomes. Building on the strong foundation laid by the 2024 English guidance Accelerating Transformation: How to Develop Effective NHS-Industry Partnerships, these resources are designed to help teams navigate the practicalities of partnership working with confidence, ensuring ethical robustness, local relevance, and measurable benefits for all involved.
Our shared aim is to equip NHS organisations in Wales and industry partners with the tools, clarity, and confidence to deliver high-quality, patient-centred projects that address real needs, respond to local priorities, and can be scaled when successful. By setting out clear steps, templates, and checklists, this guidance helps to remove barriers, reduce complexity, and create the space for innovation to flourish.
Above all, it is an invitation to think ambitiously about what partnership can achieve in Wales and to act on that ambition. We encourage those working to improve health in Wales to use this guidance as a springboard for action, building collaborations that turn potential into progress and progress into lasting, measurable impact for patients, communities and the health system.
 Darren Hughes
Darren HughesWelsh NHS Confederation
 Dr Richard Torbett
Dr Richard TorbettABPI
At a glance: How to develop effective HSC-industry partnerships
Who this guidance is for
Healthcare organisations in NI, industry leaders and those leading on the partnership and transformation agenda within their organisation or system.
Use it to:
bring stakeholders and partners together to assess priorities
design and implement partnership projects aligned to strategic objectives and informed by the guidance resources
strengthen assurance and nurture the culture of effective partnership working
scale existing partnerships across care settings.
Project identification and scoping
Key activities
Identify unmet need: Healthcare organisations and industry partners identify unmet needs to support improved clinical outcomes and explore how collaborative working and joint working projects can assist. This process includes community engagement and patient feedback to identify opportunities for improvement.
Assess scope: Undertake assessment of the project scope and aims to help identify whether a project is a collaborative or joint working project.
Agree objectives and timescale: Outline the project’s purpose, objectives, resource impact and timelines – to be approved by parties to enable progression to Stage 2, the project setup stage.
Project setup and governance structures
Key activities
Form project team: Project team or steering committee is formed.
Build trust: Work undertaken to engender trust and ethos of effective partnership working.
Develop project initiation document (PID): Develop and approve a project initiation document (PID) that details the aims and objectives of the project, expected outcomes, project completion date, exit strategy, project organisational structure, resources as well as data and patient protection.
Governance frameworks: Establish project governance arrangements
Engage with stakeholders: Undertake stakeholder engagement relevant to the project setup.
Certify PID: PID developed and agreed with the healthcare organisation, project team, governance committee and industry partner respectively. It must then be certified by the industry partner.
Publish executive summary: An executive summary of the project rationale, period, objectives, roles and responsibilities of the parties, and financial arrangements must be published on the industry partners website before arrangements are implemented. It should be certified by the industry partner.
Project implementation and outcomes reporting
Key activities
Deliver project: Project delivery and evaluation.
Monitor progress: Project monitoring and regular reporting against outcomes outlined in the PID and within the written agreement. If significant changes to the project occur during implementation, an amendment framework should be completed and agreed by the project team and the governance committee.
Publish project outcomes: All parties should publish outcomes of the project within six months of completion.
Disclosure UK: Transfers of value related to projects must also be disclosed via
Deliver project: Project delivery and evaluation.
Monitor progress: Project monitoring and regular reporting against outcomes outlined in the PID and within the written agreement. If significant changes to the project occur during implementation, an amendment framework should be completed and agreed by the project team and the governance committee.
Publish project outcomes: All parties should publish outcomes of the project within six months of completion.
Disclosure UK: Transfers of value related to projects must also be disclosed via the Disclosure UK database.
The 2024 ABPI Code of Practice exists to regulate the promotion of prescription medicines to UK health professionals, industry interactions with health professionals, and the provision of information about prescription-only medicines to the public.
About this guidance
This guide provides a practical, step-by-step resource to help the NHS in Wales and pharmaceutical industry develop, deliver and evaluate partnerships that will drive improvements to the health and wellbeing of patients in Wales. It contains templates, recommended frameworks, and handy checklists and prompts to support you.
It contains template forms, recommended frameworks, and handy checklists and prompts to support you.
Access downloadable, editable documents wherever you see the icon.
Who this guidance is for
This document is aimed at NHS organisations in Wales, pharmaceutical industry leaders, and those leading on the partnership and transformation agenda within their organisation or system.
We want you to use it to:
bring stakeholders and partners together to assess priorities for NHS-industry partnership working
design and implement partnership projects aligned to strategic objectives and informed by the guidance resources
strengthen assurance and nurture the culture of effective partnership working
scale existing partnerships
across care settings
What are NHS-industry partnerships?
NHS-industry partnerships allow NHS organisations and the pharmaceutical industry to collaborate for patients’ benefit. Joint working was recognised by the Welsh Government when it issued a Welsh Health Circular (WHC) in 2005 ‘Guidance for partnership working between NHS organisations, primary care contractors, the pharmaceutical industry and the allied commercial sector in Wales’.1
Collaborative working is generally between one or more pharmaceutical companies, healthcare organisations and possibly other organisations. It must have, and be able to demonstrate, the pooling of skills, experience and/ or resources from all parties involved. There must be a shared commitment to successful delivery from everyone involved and each organisation must make a significant contribution. In the case of NHS organisations, this contribution does not have to be financial. It can involve the sharing of support in the form of skills and experience to deliver projects successfully.
Joint working projects are a specific type of NHS-industry collaborative working, rather than a generic term for all cross-sector collaboration. They must be patient-centred and always benefit patients directly, which gives them a narrower focus than collaborative working.
Since then, multiple publications have acknowledged the value of external expertise in helping NHS organisations overcome challenges. This includes providing additional skills and resources to achieve patient benefits beyond that which NHS organisations could deliver alone. These partnerships bring industry skills and expertise to improve appropriate patient access to innovative treatments, support project management and enhance the efficient delivery of healthcare services.
Partnerships can be formed between a single NHS organisation and a single pharmaceutical company, or multiples of either. In general, there is a trade-off between the advantages of greater scale in working with multiple partners, as seen through regional working in Wales, and the added complexity of gaining agreement across multiple organisations.
While patient organisations cannot directly be included in collaborative working arrangements, they may be contracted to deliver a service to support an element of such collaborative working.
There are two types of NHS-industry partnership: collaborative working and joint working projects. These partnerships involve cooperation between industry and local NHS organisations across primary, secondary and system-level healthcare settings.
The benefits of working together
Collaborative and joint-working approaches: a comparison
As noted in the comparison table, one of the key benefits of collaborative working is the ‘triple-win’ - benefiting patients, healthcare organisations including the NHS, and pharmaceutical companies. Benefits for pharmaceutical companies in embarking upon collaborative working can be myriad, from gaining experience in partnering with an NHS organisation, to an increase in patient identification and prescribing in accordance with national and local guidelines. Most importantly however, and in accordance with Clause 20 of the ABPI Code of Practice, such benefits must not constitute an inducement to health professionals or other relevant decision makers to prescribe, supply, recommend, buy or sell a medicine. A key safeguard here is the requirement in the ABPI Code of Practice to have a have a summary of the collaborative working agreement publicly available before arrangements are implemented.
It is also worth noting that in embarking upon collaborative working with NHS organisations, companies will have no direct contact with patients, or with identifiable patient level data.
| Collaborative-working projects | Joint-working projects |
|---|---|
| Are for the benefit of patients and/or the healthcare organisation, including the NHS. | Must always be for the benefit of patients directly and must include the NHS as a party. |
| Enhance patient care or be for the benefit of patients, or alternatively benefit the NHS and, as a minimum, maintain patient care. | |
| May not constitute a grant/donation (see Clause 23 of ABPI Code of Practice for further information on Donations and Grants). | |
| May provide benefits to the company or companies involved. |
|
Outcomes must be defined in such a way that they can be measured or tracked, so that at any time during the collaboration all parties are aware of:
|
|
| Must be carried out in an open and transparent way, with a certified summary of the project agreement publicly available before it begins. | |
| Must respect clinical independence. | |
| Must be prospective – not relating to a project that has already begun. | |
| Must have the value to the healthcare organisation publicly disclosed annually on the Disclosure UK database and, if relevant, the contracted service value to the patient organisation published on the industry partner’s website. | |
| Must not constitute an inducement to health professionals or other relevant decision-makers to prescribe, supply, recommend, buy or sell a medicine. | |
| Must ensure that the rights and legitimate interests of all parties are continuously observed throughout, including considerations related to data security, the protection of confidentiality and privacy, and anti-bribery compliance. | |
| Must not promote a prescription-only medicine to any member of the public. | |
Partnerships offer a proven ‘triple win’ — improving outcomes for patients, strengthening the health system, and supporting responsible industry innovation. In Wales, where health inequalities, service variation, and workforce pressures remain major challenges, these partnerships offer a strategic opportunity to accelerate transformation:
Equitable and evidence-based prescribing
Evidence indicates that NHS organisations engaged in industry partnerships are up to 2.5 times more likely to follow NICE-recommended prescribing for clinically and cost-effective medicines, especially in areas like cardiovascular care. This is particularly pertinent in Wales, where prescribing practices can vary across health boards. Partnership working helps standardise treatment approaches and improve consistency in care.
Improving Outcomes and Reducing Inequalities
Partnerships across the UK have helped align clinical practice with national guidance and guidelines, improved access to diagnostics and treatments, and reduced unwarranted variation – benefits that are especially meaningful in Wales, where health outcomes often correlate with levels of deprivation.
Capacity and Capability for Transformation
As demonstrated by The King’s Fund, partnerships deliver more than just resources – they create space for innovation by funding project management, analytics, and digital tools, enabling frontline clinicians to lead sustainable service redesign. This external support is particularly valuable in the Welsh context, where health boards and trusts often operate with limited headroom for service improvement while balancing day-to-day operational pressures.
The ABPI Code of Practice
The 2024 ABPI Code of Practice exists to regulate the promotion of prescription medicines to UK health professionals, industry interactions with health professionals, and the provision of information about prescription-only medicines to the public.
It is administered by the Prescription Medicines Code of Practice Authority (PMCPA) and is the cornerstone of the UK system of industry self-regulation. All NHS-industry partnerships are bound by the ABPI Code of Practice.
“Partnerships have to operate within the safeguards of the ABPI Code of Practice, which reflects and goes beyond the law. This means partnerships take place in an ethical and transparent manner, which puts patients at the heart of everything we do.” Dr Amit Aggarwal, Executive Director, Medical Affairs and Strategic Partnerships, ABPI

Multi-partner considerations
Collaborative working projects between a single healthcare organisation and a single pharmaceutical company are common. Less common but still possible are cross-sector projects involving more than one healthcare organisation and/or more than one pharmaceutical company.
Cross-sector projects between one or more healthcare organisation and one or more pharmaceutical company are often more complex. This is because each individual organisation has its own governance and approvals processes, which can lengthen the timelines for project set-up and implementation. In addition, ABPI members are actual or potential competitors in certain therapy areas and are therefore subject to stringent competition law safeguards that must also be reflected in any agreement on working together. A shared desire to improve patient outcomes through a collaboration will not justify anticompetitive conduct, such as the illegal exchange of sensitive information between competitors or other types of collusive practices. Multi-partner considerations
There should be a lead contracting party, identified by job role, in each sector in a cross-sector project where there are multiple healthcare organisations or to have an individual contract with each organisation involved.
Where there is more than one contracting party on each side of the cross-sector project, steps should be taken to understand the differing legislative competence, governance processes and timelines involved.
Given that the legal risk and opportunities for error are higher when multiple organisations are involved in the same collaboration, it is best to agree rules of engagement upfront, which can be recorded in the agreement. Such rules should set out clear governance principles, such as:
- All project meetings will only take place if at least one representative of each party can attend
- Minutes of all meetings will be taken, approved by all participants, and kept on record for an agreed period after the completion of the project
- All project participants will receive a briefing on competition law rules and will be asked to sign a competition compliance and non-disclosure statement.
If the nature of the project would require specific discussion on topics of the utmost sensitivity such as costs, patient information, potential tendering opportunities, R&D activities etc., the parties should consider having a specialist competition lawyer attend the meetings.
Key stages of the project lifecycle
The figure below outlines the stages of a partnership, from planning to delivery and monitoring:
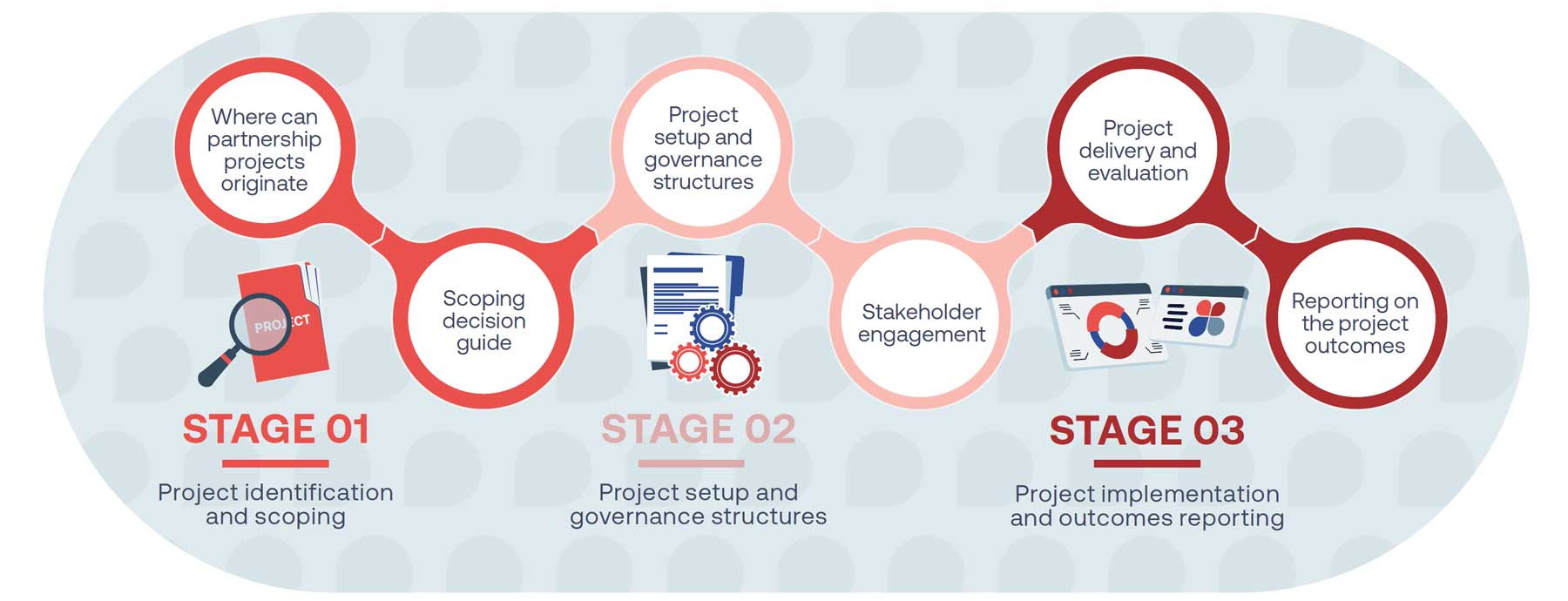
Stage 1 Project identification and scoping
and scoping
““Across Wales, NHS leaders are working hard to improve care and health outcomes for patients, while seeking to reduce inequalities. When industry and NHS organisations develop effective partnerships, there are significant benefits for all concerned – higher quality care, lower hospital admissions and more appropriate use of medicines.
We want to help more people in Wales benefit from this triple win. The joint Welsh NHS Confederation and ABPI guidance will support teams to confidently collaborate in the interest of their local communities.””
Welsh NHS Confederation
Where can partnership projects originate?
In Wales, partnerships can originate from across the NHS in Wales, as well as from the pharmaceutical industry. The table below sets out some suggestions. Both parties can discuss initial project ideas with the Life Sciences Hub Wales.2
| Primary care | Secondary care | Integrated care system/ place level | |||
|---|---|---|---|---|---|
|
Primary care or cluster partnerships often arise from existing relationships with industry providers. At other times, they will emerge from proactive work by the clusters or individual practices who are interested in finding partners to support specific projects. Industry partners will also often research and directly scope out primary care providers where projects can directly support their existing clinical priorities. |
Across secondary care settings, partnership working is well established, and as such clearer routes exist for projects to be developed. In many cases, agreed avenues for exploring partnerships are in place, such as via relationships between industry and trusts, as well as dedicated commercial services teams who will issue expressions of interest regarding partnership objectives and opportunities. This is further enhanced by the wealth of existing secondary care networks, which enable a greater spread of successful projects from one locality to another. |
Partnership working with Health Boards (HBs) can be more challenging to establish. It is important therefore that any prospective partnership is underpinned by mission-oriented priorities that directly support the system’s regional obligations and local objectives. Early-stage discussions about entering a collaborative or joint working arrangement with LHB staff should include relevant clinical leads and executive leads, including the Chief Pharmacist as appropriate. If proposals are deemed suitable for further exploration, it is advised that the designated NHS and industry leads should provide initial details on the scope and aims for consideration by the relevant Board level working groups. The NHS Wales Performance and Improvement (previously NHS Wales Executive) and Life Sciences Hub Wales, who operate separately from the LHBs in Wales, can also serve as an important conduit for streamlining the setup of system-level partnerships aligned to system priorities. |
|||
Key resource: Scoping decision guide
At the start of a partnership, NHS and industry organisations need to identify unmet needs to support clinical outcomes. Industry partners often align their capabilities with NHS goals or issues identified through health data analysis.
This process includes community engagement and patient feedback to identify opportunities for improvement. Colleagues should use these questions to explore and develop the scope of a project, to ensure the aims are clear and the entire lifecycle of the project has been considered.
| Questions to consider during the scoping of a project | Questions to consider if the project has a therapy/medicine focus |
|---|---|
| What is the unmet need the project is seeking to address? | Which clinical pathway(s) require service redesign to improve patient care and/or system improvement? |
| What is the scale of the problem? | |
| What is the evidence to back this up? | Which companies have expertise in this area? |
| What is the priority improvement area, and can this realistically be addressed within the resources and duration of the project? | |
| What are the patient or system benefits of addressing this need? | Are there other organisations that would be relevant to engage in the project? For example, at an ICS level, can HINs play a convening and facilitation role for the partnership? |
| What would be the impact on patient care or the system if this need is not addressed? | |
| Are other internal stakeholders supportive of addressing the need and the feasibility of doing so? | |
| Which NHS plan and/or local improvement plan goal is the challenge aligned to? | |
| What interventions are required and in what timescale? | How are partners considering the impact of health inequalities and equality of healthcare access? |
| What is the likely impact on the clinical and non-clinical workforce? For example, will this project involve complex pathway redesign? |
|
| Are prospective partners clear on existing operational pressures, and their potential impact on the project? |
|
| What related challenges need to be addressed in other parts of the system for the project to succeed? |
|
| What does success look like? How will it be measured? When and by whom? | |
| Is the project intended to demonstrate a sustainable solution? If so, what outcomes will be necessary to ensure a successful business case? |
|
| Is there capacity to release the necessary internal team members to participate in the project? |
Key resource: Checklist for determining if a project is collaborative working, joint working or neither
To help identify if a project is a collaborative or joint-working project, an
assessment of the project scope and aims should be undertaken, which can be supported by completing the checklist below.
If the answer to any red questions on the checklist is ‘No’, the project is not a collaborative or joint–working arrangement, and will need to be modified before proceeding. If changes cannot be made, prospective partners should consider an alternative approach, such as a research collaboration or a donation/grant, as described in Clause 23 of the ABPI Code of Practice.
If the answer to any amber questions is ‘No’, this signals an issue or risk that should be addressed to encourage successful and timely project delivery.
| Joint working | ||
|---|---|---|
| 1A. Is the main benefit of the project focused on the patient? | YES This is a joint-working project – go to question 2 (page 17) |
NO Please go to question 1B |
| Collaborative working | ||
| 1B. Does the project aim to enhance patient care or be for the benefit of patients, or alternatively benefit the NHS and, as a minimum, maintain patient care? | YES This is a collaborative-working project – go to question 2 (page 17) |
NO Consider another form of support |
| Red questions | |||
|---|---|---|---|
| # | Question | YES | NO |
| 2 | Do all parties acknowledge that the arrangement may benefit the NHS and company partner(s) involved? | YES | NO |
| 3 | Are any subsequent benefits at an organisational level and not specific to any individual? | YES | NO |
| 4 | Is there a significant contribution of pooled resources from all parties, which include people, finance and equipment wholly or partly dedicated to the project? | YES | NO |
| 5 | Is there a shared commitment to joint development, implementation and successful delivery? | YES | NO |
| 6 | Will anonymised, aggregated, outcome data be measured and documented? | YES | NO |
| 7 | Are all partners committed to publishing a measured and documented executive summary of the Collaborative Working Agreement? | YES | NO |
| 8 | Are all proposed treatments involved in line with national guidance, where it exists? | YES | NO |
| 9 | Will all activities be conducted in an open and transparent manner, with appropriate governance arrangements in place to manage any conflicts of interest? | YES | NO |
| 10 | Has an exit strategy and any contingency arrangements been agreed? | YES | NO |
| Amber questions | |||
|---|---|---|---|
| # | Question | YES | NO |
| 11 | Will the project be managed by a team including representatives of industry, the NHS and appropriate third-party representation? | YES | NO |
| 12 | Do all parties and their respective organisations have the appropriate skills, capabilities and capacity to manage the project? | YES | NO |
| 13 | Have all partner organisations got clear procedures in place for reviewing and approving collaborative-working projects? | YES | NO |
| 14 | Are all parties committed to working together across the entire lifecycle of the partnership? | YES | NO |
| 15 | Are all partners clear on who within their organisation is responsible for ensuring that relevant joint-working / collaborative-working documents are certified or approved? | YES | NO |
Key resource: Project Concept Framework
The key recommended documentation for stage 1 is a Project Concept Framework, outlining the project’s purpose, objectives, resource impact and timelines. It must be approved by all relevant parties to support progression to the project setup stage.
Stage 2 Project setup and governance structures
and governance
structures
“It is often difficult building and managing
successful partnerships, with those involved
facing time constraints and complex challenges
when seeking to innovate or work in new
ways. The guidance set out by the Welsh NHS
Confederation and ABPI helps to show the clear
steps that can support effective collaboration.”
Project setup and governance structures
At this stage, a project team or steering committee is formed, including all involved parties and active participants. This team will guide and manage the project, being responsible for its success and operating within the agreed limits.
The members of this project team may differ depending on the care setting. The team should be ‘right sized’ to be both effective and inclusive.
All project team or steering committee members must declare any conflicts of interest.³ Those with a conflict should not vote on related matters. These declarations should be recorded in the meeting minutes. Either party can object to someone’s involvement due to a conflict of interest.
The project team should agree on a project methodology. PRINCE2 (Projects In Controlled Environments) is perhaps the best known and most widely used, but the methodology may vary depending on the complexity of the project. The team should also agree on a regular meeting schedule to make initial decisions, keep the project on track, and manage any issues. Meetings should be action-oriented, with clear agendas, decision points, and minutes recorded.
When considering project resourcing, all parties must commit to detailing the resources they will contribute to the project, which could include finances, skills, or experience. These contributions should go beyond normal day-to-day roles, like funding additional staff or clinics. Assigning a monetary value to healthcare resources is challenging, but it should be clear that contributions from partners should be comparable and proportionate. If the collaboration aims to address organisational constraints within the NHS in Wales, precautions must be taken when using pharmaceutical funding to retain staff. Any staff paid through industry funding should operate under the control of an organisation within the NHS in Wales, be time limited and outlined in collaborative working documentation, with clear employment law compliance. Exit strategies for industry-funded posts should be outlined in project documents.
3. In the NHS in Wales, conflicts of interest are addressed through a combination of policies, guidance, and procedures. Staff are expected to declare any interests that could potentially influence their decision-making or create a conflict with their NHS duties. This includes outside employment, financial interests, and personal relationships that could create a conflict.
Key resource: Project team/steering committee members (non-exhaustive)
Who should be in a project team/project steering committee? (non-exhaustive)
| Care setting (options depending on local context) | Key stakeholders |
|---|---|
| Primary care |
Industry
|
|
|
| Secondary care |
Industry
|
|
|
| Health board |
Industry
|
|
|
Due to the non-promotional nature of collaborative working projects, careful consideration should be given to the industry stakeholder job roles within their company, particularly with regards to sales or promotional roles.
Key resource: Steps to build trust
Trust and transparency is fundamental to any partnership, especially during the early scoping phase. All parties should ensure that they work towards engendering trust, which can be supported through the following steps:
Key resource: Project initiation document (PID)
Once the necessary criteria have been fulfilled, the project team should develop and approve a project initiation document (PID) to ensure a shared understanding of the project’s outcomes, its governance framework and to provide a clear exit strategy that details the overall responsibility of each party if the project needs to be terminated.
The PID is a key document that sets out requirements ahead of project implementation and the agreed copy should be kept on record for both parties’ reference.
Confidentiality of patient information must be maintained in all partnerships, as outlined in the PID. This includes respecting the confidentiality of project-related information and not sharing it beyond the project’s scope. The PID should be collaboratively created by relevant individuals from all partnering organisations.
It is important to note that PIDs will, at times, need to be updated following the initiation of the project. This can be addressed via a project amendment form (see implementation section).
The PID must be certified by the industry partner and be approved by both the project team also the relevant governance committee(s) – see page 28 for further details.
Accelerating transformation: Project initiation document template
project. This section should also include an agreed process and timelines should it be necessary to terminate the project early.
according to employee time and resource across NHS and industry partners.
*Clause 20 of the ABPI Code states that collaborative working, including its implementation, must have and be able to demonstrate the pooling of skills, experience and/or resources from all of the parties involved for the joint development and implementation of patient and/or healthcare centred projects. There must be a shared commitment to successful delivery from all parties, and each party must make a significant contribution.
Establishing a robust governance framework
When entering into a partnership initiative, industry and organisations need to ensure they are working within a robust governance framework to ensure the project aligns with their organisations’ goals and legal processes.
Projects should include the establishment of a governance committee to oversee the project. The governance committee will also review the principles of the project against the collaborative and joint-working checklist criteria and ensure that the project has been reviewed by each participating organisation’s management and experts.
Within pharmaceutical companies, governance expertise will be provided by legal, medical, compliance and healthcare engagement functions.
Within healthcare organisations, governance will usually be provided by existing governance committee, or other appropriate committee, such as an Internal Review Committee (IRC). For collaborative projects, stakeholders must have the authority to approve the project.
Examples of key individuals who can form part of a governance committee are presented alongside:
Key resource:
Potential governance committee members across care settings (non-exhaustive)
- Named executive senior responsible officer from each party to the partnership
- Relevant clinical lead
- Programme management and support
- Insight and intelligence teams
- Pharmaceutical legal director
- Pharmaceutical medical / compliance director
Stakeholder engagement
Building confidence in the project with stakeholders, both internal and external, is vital to avoid misunderstandings and ensure transparency.
This includes clarifying aligned interests and disclosing benefits to industry transparently. Clear communication between partners is essential to refine project objectives, manage expectations and confirm inputs from each organisation. At this stage, the project team should develop a stakeholder map, communications plan and data collection plan if not already done in the PID. Realistic timescales should be set, with the first three steps taking four to six months, including scoping, development and approval of governance arrangements and legal framework.
It is a helpful exercise to divide stakeholders between internal and external stakeholders who:
- should be involved in the project
- are not directly involved in the project, but whose views could influence the outcome and who should be kept informed throughout the entire project lifecycle
- will ultimately be impacted by the outcome
- whose opinions could facilitate or prevent success.
Key resource: Examples of stakeholder groups to engage across care settings (non-exhaustive)
| Primary care | GPs, pharmacists, patients and communities, patient organisations |
| Secondary care | Chair of Quality Committee, Chair of Medicines Optimisation Group, patients and residents, patient organisations |
| System-level care | Chair of Quality Committee, patients and residents, patient organisations |
| Industry | Company decision makers, local representatives, market access teams, project managers |
| Others | NHS Wales Performance and Improvement, Welsh Government |
Patient engagement
NHS organisations and pharmaceutical industry partners should give due consideration to the impact on patients, and if appropriate, gain feedback from patients or patient groups.
Ways to incorporate patients' views and experiences can include:
- Patient stories of their experiences
- Mapping the key pathways of service with patients and staff working in coordination
- Considering community representation so that plans being developed represent diversity and the needs of different groups impacted, and ensuring inequalities are considered
- Recording a patient’s experience of a service and asking for their views following the completion of the project for inclusion in the project outcomes.
Key resource: Recommended Collaborative/Joint Working Agreement Framework
Once the project has been approved in principle by all relevant parties, the project team must work with its organisational legal experts to draft and sign a Collaborative/Joint Working Agreement. The agreement is a legal contract that will include key information about the project and plans, drawn directly from the PID. It must be entered into with legal, corporate entities and not with any individual in primary, secondary and system-level settings.
The agreement must ensure that any confidential, competitive or personal data are protected by strong contractual provisions. It should include the following:
- The name of the collaborative-working project, the parties to the agreement, the date and the term of the agreement
- Aims and objectives
- Considering community representation so that plans being developed represent diversity and the needs of different groups impacted and ensuring inequalities are considered
- The expected benefits for patients, the population or user groups, the NHS or other healthcare organisation, the pharmaceutical company and other organisation(s) as applicable
- Principal activities and accountabilities
- Composition of the steering group / project group
- Timelines and project milestones
- Description of pooled resources
- Financial arrangements
- Roles and responsibilities of the healthcare organisation, the pharmaceutical company and other organisations
- How the success of the project will be measured, when and by whom
- Relationship, if any, to the company’s or companies’ medicine(s)
- An executive summary of the project which will be published on the industry partner’s corporate website before the project begins
- Process for project amendment
- Dispute resolution clause
- Defined exit strategy (for all parties)
- Contingency arrangements to cover unforeseen circumstances (e.g. updated guidance or product summaries)
- Agreement on intellectual property rights following completion of the project
- Data management and data sharing plans
- Pharmacovigilance plans (if required)
- A plan to publish project outcomes within six months of completion to support wider learning
- A commitment to disclose transfers of value to healthcare organisations via Disclosure UK
Please note: Any collaborative or joint-working agreements must be entered into with legal, corporate entities and not with any individual member of staff across primary, secondary and system-level settings.
The executive summary
The last stage in the project setup is the publication of an executive summary, which will largely draw from the content in the collaboration working agreement.
As outlined in the ABPI Code of Practice, a summary of the collaborative working agreement (executive summary) must be published on the pharmaceutical company’s or companies’ website before arrangements are implemented. It is also advisable that relevant NHS partners do the same. The project should not commence until the executive summary has been published on the relevant industry partner(s)’ website. A recommended executive summary framework is shown in the key resource.
Key resource: Recommended Collaborative/Joint Working Project Executive Summary Framework
Accelerating transformation: collaborative / joint working executive summary template
Stage 3 Project implementation and outcomes reporting
and outcomes
reporting
“I have seen first-hand the benefits of NHSindustry collaboration for patients, staff, the NHS and the local economy. In the face of the myriad challenges facing health and care services and our patients, we must find new ways to drive improvement and transformation for our local communities.
The NHS alone does not have all the answers, so responsibly using industry partners with expertise and additional resource is key to ‘doing things differently’ if we want to see real change. Tackling the barriers we know leaders on both sides face will ensure we are best placed to seize these opportunities.”
Hywel Dda University Health Board
Project delivery and evaluation
Once the collaborative agreement is signed and published on the industry partners’ website, the project officially starts.
To monitor project progress effectively, partners should refer to the outcomes outlined in the PID and executive summary.
Collaborative and joint-working projects are not set up as clinical trials or real-world evidence-generating trials, and as such, the project metrics need to be realistic and based upon the objectives of the project and intended purpose thereafter, ie business case or scalable solution. Examples of relevant metrics include clinical impact, delivery, service effects and economic impact. After project completion, outcomes will be measured and documented, with stakeholders and the project team evaluating learnings from the project.
Key resource: Project monitoring guidance
If significant changes to the project occur during implementation, the following form should be completed and agreed by the project team and the governance committee in order to keep a record of the project aims as part of good governance:
Key resource: Recommended Project Amendment Framework (for use only if necessary)
Reporting on the project outcomes
It is important to recognise that successful organisations will learn from their experiences of partnerships.
Learning is more beneficial when it is preserved beyond the end of the project in the outcome report. As well as evaluating the outcome of the project, it is useful to assess how successful or unsuccessful the operation of the project has been so that lessons can be learned and can be usefully applied in the design and running of other projects.
As stated in the ABPI Code of Practice, all parties should publish outcomes promptly, within six months. Local NHS organisations are encouraged to do the same. To promote and expand successful collaborations in healthcare, these outcome reports should be shared with ABPI for their NHS-Industry Partnership Case Studies Library to support more partnerships.
To ensure that partnerships are transparent, transfers of value related to collaborative projects must also be disclosed via the Disclosure UK database (see Appendix 2 for further details on Disclosure UK, including how any contracted service values to patient organisations are disclosed).
Key resource: Recommended Summary of Project Outcomes Framework
Summary of project outcomes: template
| Summary of project outcomes – template | |
|---|---|
| Project name | Include a short sentence that outlines the project title. |
| Project partners | Outline the partnering organisations that took part in the collaboration. |
| Duration | Detail the project initiation and completion dates to the nearest month, e.g. December 2025 – July 2026. |
| Project overview | Provide an overview of the project, including its objectives and how the project set out to achieve them. |
| Project outcomes | Outline the results from the project, including benefits to patients, the NHS, and industry. This section should address the following:
|
| Conclusions and learnings | Include the conclusions and learnings drawn from the project, with the aim of supporting learnings for other projects. |
| References | Include here examples of any NHS or National Institute for Health and Care Excellence (NICE) or All Wales Medicines Strategy Group (AWMSG) policies that are relevant to the project. |
Further reading
Previous ABPI/NHS Confederation publications
- Collaborate to Innovate: Learning from NHS, Charity and Life Sciences Industry Experience to Build a Culture of Research and Innovation in the UK (April 2024)
- Partnering with Purpose: How Integrated Care Systems and Industry Can Work Better Together (November 2023)
- Transforming Lives, Improving Health Outcomes: Tackling the True Cost of Variation in Uptake of Innovative Medicines (January 2023)
Historic partnership guidance
- Working Together - A guide for the NHS, Healthcare Organisations and Pharmaceutical Companies (April 2022)
- Joint Working - A Toolkit for Industry and the NHS (September 2019)
- Simplifying cross-sector working between NHS Integrated Care Systems, Sustainability and Transformation Partnerships and industry: Guidance on governance and process (May 2019)
- Joint Working – A Quick Start Reference Guide for NHS and Pharmaceutical Industry Partners (2012)
- Moving Beyond Sponsorship – Joint Working Between the NHS and Pharmaceutical Industry (August 2010)
- Best Practice Guidance on Joint Working Between the NHS and Pharmaceutical Industry and Other Relevant Commercial Organisations (February 2008
- Collaborative Working and Joint Working: A toolkit for industry and NHS Wales
Additional reading
- Guide to collaborative working between NHS, primary care contractors and the pharmaceutical industry
- A Common Understanding 2025 Working Together for the People of Scotland
- The King's Fund: NHS and life sciences industry partnerships: collaborating to improve care
- Partnering for progress: a data-driven analysis of NHS-industry partnerships
Appendices 1 and 2
Appendix 1: The ABPI Code of Practice
The 2024 ABPI Code of Practice exists to regulate the promotion of prescription medicines to UK health professionals, industry interactions with health professionals, and the provision of information about prescription-only medicines to the public, including patients and patient organisations.
It is administered by the Prescription Medicines Code of Practice Authority (PMCPA) and is the cornerstone of the UK system of industry self-regulation.
All NHS-industry partnerships are bound by the code, which serves as a guardrail by which industry is regulated to ensure that throughout all collaborations, patient safety is maintained, in a professional, ethical and transparent manner to ensure the appropriate provision of high-quality care. At its heart, the code gives confidence to local NHS organisations that partnerships operate in a clear and robust framework.
Strong support is given to the code by the industry with all companies devoting considerable resources to ensure that their activities comply with it. Any complaint made against a company under the code is regarded as a serious matter both by that company and by the industry as a whole. Sanctions are applied against a company ruled in breach of the code.
Underpinning this are the ABPI Principles, which sit alongside the code. These set out the behaviours that embody the spirit of the code, and the ABPI expects that companies build these into their culture and approach.
The four key principles are as follows:
- Commitment to benefiting patients and ensuring patient safety by operating in a professional, ethical and transparent manner to ensure the appropriate and rational use of medicines and to support the provision of high-quality healthcare.
- Acting with integrity and committing to relationships that are responsible, professional, ethical and transparent.
- Commitment to ensuring that transparency is respected.
- Interacting with all stakeholders with respect.
The ABPI Code reflects and extends beyond relevant UK legislation and ensures that the ABPI meets its commitments to implement other codes, such as those from the International Federation of Pharmaceutical Manufacturers and Associations and the European Federation of Pharmaceutical Industries and Associations Codes.
The code is also supplemented by Disclosure UK, a Europe-wide initiative to increase transparency between pharmaceutical companies and the organisations they work with. Further information on Disclosure UK can be found in Appendix 2.
Appendix 2: Disclosure UK
The relationship between the pharmaceutical industry, healthcare professionals and healthcare organisations plays a vital role in the development of life-enhancing and life-saving medicines.
At the core of the relationship is sharing knowledge to improve patient outcomes. To ensure this relationship is open and transparent, the pharmaceutical industry has taken the lead on disclosing ‘transfers of value’ – payments and benefits-in-kind – made by industry to healthcare professionals and healthcare organisations through Disclosure UK, a publicly searchable database hosted by the ABPI.
Disclosure UK is part of a Europe-wide initiative to increase transparency between pharmaceutical companies and healthcare professionals and organisations.
Data shown on Disclosure UK covers:
- Participation in advisory boards
- Speaking at or chairing meetings
- Working with and advising doctors and scientists in pharmaceutical companies
- Speaking at conferences and symposia
- Attendance at national and international conferences
- Medical education and training funded by companies
- Provision of grants and donations to healthcare organisations
- Sponsorship of healthcare education events
Details of collaborative and joint working projects with healthcare organisations are also disclosed individually on the database. Certain research and development transfers of value to healthcare professionals, decision makers, and healthcare organisations are also disclosed in aggregate.
Separately, companies must disclose transfers of value made to patient organisations and fees for contracted services to members of the public, including patients and journalists.
The ABPI Code requires that this information is published on company websites with gateway links to Disclosure UK.
For more resources or to search the database, visit: www.disclosureuk.org.uk
These disclosure requirements are in addition to:
- An executive summary of each project published on the industry partner’s website before project start.
- Outcome publications within six months of project completion by all partners.
-
ThemeDevolved Nations - Cymru Wales
-
KeywordsDevolved Nations - Cymru WalesWales
-
PublisherWelsh NHS Confederation, ABPI
